Introduction to RTSA and Study Background
The reverse total shoulder arthroplasty (RTSA) has revolutionized the treatment of rotator cuff tear arthropathy, massive irreparable rotator cuff tears, glenohumeral osteoarthritis with rotator cuff compromise or glenoid bone loss, acute and chronic sequelae of proximal humeral fractures, and revision shoulder arthroplasty. As a non-anatomic arthroplasty, RTSA continues to generate debate regarding ideal implant positioning to optimize patient outcomes. Implant position directly impacts shoulder function, influencing component stability, overall joint stability, impingement-free arc of motion, and muscle efficiency. In this context, Maxwell and colleagues recently published, “The effect of reverse shoulder arthroplasty…” in the Journal of Shoulder and Elbow Surgery.2 Within this study, 10 arthroplasty surgeons planned 20 arthroplasties (10 glenohumeral osteoarthritis and 10 rotator cuff tear arthropathy) with three prosthesis configurations. The authors here have performed a purely computational analysis, so the clinical impact remains theoretical.
Implant Configurations and Design Styles
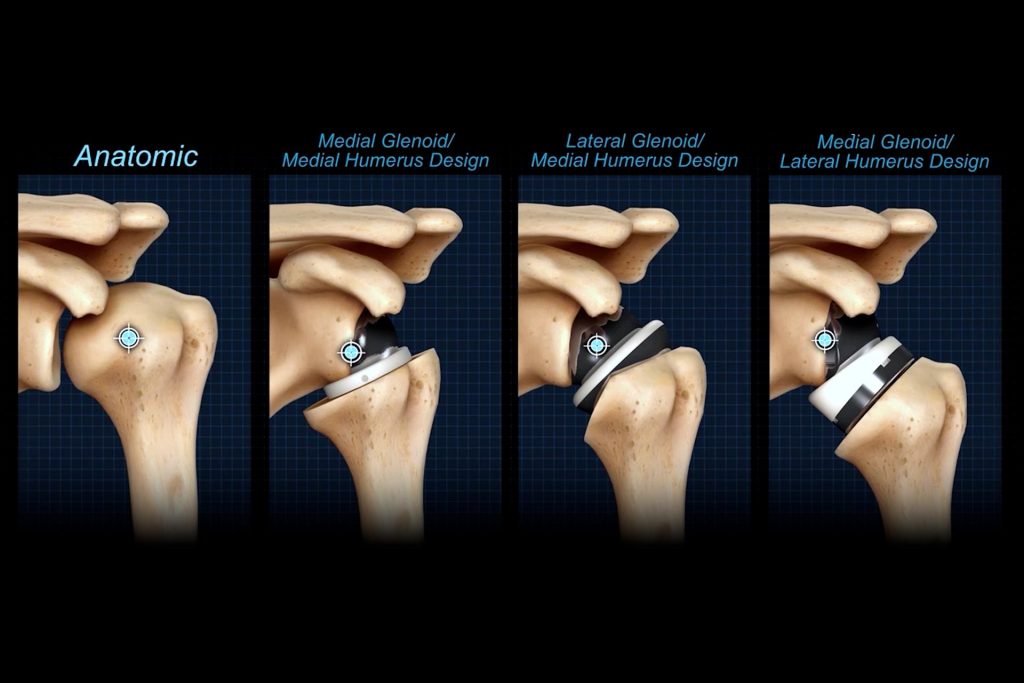
The configurations tested reflect compromises between glenoid lateralization and humeral neck-shaft angle. The first configuration included an 8mm lateralized glenosphere with a 135° neck-shaft angle humeral component [135+8], which best replicates a “Frankle” style implant. The second configuration included a 4mm lateralized glenosphere with a 145° neck-shaft angle humeral component [145+4], representing a “compromise” style implant. The third configuration included a 0mm lateralized glenosphere with a 155° neck-shaft angle humeral component [155+0], representing a “Grammont” style implant.
Methodology and Anatomical Starting Points
The authors then compared percentage change in length and post-operative lengths for deltoid, infraspinatus, subscapularis, and teres minor between these configurations. Because the study compares pre- and post-operative measurement, the inclusion of both glenohumeral osteoarthritis and rotator cuff tear arthropathy is a critical aspect as these pathologies differ in their starting positions; as rotator cuff tear arthropathy typically includes superior migration of the humeral head, while glenohumeral osteoarthritis often involves medial migration of the humeral head. These findings are reflected within the author’s dataset.
Analysis of Muscle Length Outcomes
The authors found that rotator cuff muscle lengths increased from 155+0 to 145+4 to 135+8. However, all constructs on average, decreased infraspinatus and teres minor lengths, even the 135+8 constructs. The 135+8 construct actually lateralized the middle and superior subscapularis beyond the start point, while all other constructs, on average, decreased subscapularis lengths. On average, all constructs increased deltoid length; with the largest increases observed with the 155+0 construct. However, there were no significant differences between the 145+4 and 135+8 constructs in deltoid lengths in all three heads.
The study has multiple limitations. First and foremost, the differences the authors describe are of uncertain clinical significance. For instance, does 2% shortening vs. 8% shortening of the infraspinatus alter external rotation power or motion? The study cannot answer this question. Second, the study had a limited sample size. Third, the 135° humeral component differed in geometry from the 145° and 155° humeral components. Fourth, the study is conducted statically on CT scans that were not obtained in a uniform glenohumeral position. Fifth, muscle insertions were represented as single points and modeled as linear paths, potentially underrepresenting the complexity of native anatomy.
In conclusion, this muscle modeling study demonstrates that when comparing the most critical muscle, the deltoid 135° and 145° implants may not differ significantly in deltoid length and that NSA could be selected to optimize this variable.
References
- Bacle G, Nové-Josserand L, Garaud P, Walch G. Long-Term Outcomes of Reverse Total Shoulder Arthroplasty. J Bone Jt Surg. 2017 Mar 15;99(6):454–461. PMID: 28291177
- Maxwell MJ, Glass EA, Bowler AR, Koechling Z, Lohre R, Diestel DR, McDonald-Stahl M, Bartels W, Vancleef S, Murthi A, Smith MJ, Cuff DJ, Austin LS, Wiater JM, Chamberlain A, Kirsch JM, Bishai SK, Favorito P, Chalmers P, Le K, Jawa A. The Effect of Reverse Shoulder Arthroplasty Design and Surgical Indications on Deltoid and Rotator Cuff Muscle Length. J Shoulder Elb Surg. 2024; PMID: 39638109